
I broke my clavicle - now what?
The clavicle, or collarbone, is one of the most commonly fractured bones. It represents 5% of all fractures and represents up to 45% of all fractures around the shoulder. The most common type of fracture is the middle shaft fracture. National data shows that more than 85% of patients never see an orthopaedic surgeon after being diagnosed in the hospital.
Treatment options include a sling or brace versus surgery with a plate and screws or rod. For nondisplaced fractures, where the bones are perfectly aligned, the recommended treatment is  nonsurgical. In the past, doctors treated these in a figure 8 brace to hold the shoulders back and maintain
alignment. However, over time we have learned that a simple sling offers better comfort with the same rate of healing and prevents the shoulder from sagging and the fracture from moving.
nonsurgical. In the past, doctors treated these in a figure 8 brace to hold the shoulders back and maintain
alignment. However, over time we have learned that a simple sling offers better comfort with the same rate of healing and prevents the shoulder from sagging and the fracture from moving.
Over the last decade, our understanding of the long term outcome of clavicle fractures has changed the way we treat our patients. In the past, the mantra of treating clavicle fractures has been they heal “…without the doctor, with the doctor and despite the doctor.” We now know that is not true. Over the past seven years, 32 research studies have concluded that surgical repair for displaced (out of alignment) fractures of the clavicle yields better results than nonsurgical treatment in a sling. Recent research shows that nonsurgical management of clavicle fractures have a higher nonunion rate (doesn’t heal) and lower patient satisfaction.

Some fractures will heal but in poor alignment (malunion) that can lead to significant long terms problems including:
- Pain
- Weakness
- Cosmetic deformity
- Neurological symptoms such as numbness
Traditional surgical treatment for clavicle fractures has been plates and screws. Surgical treatment of displaced clavicle fractures has been shown to demonstrate faster healing times, with an anatomical alignment and overall better outcome for patients.
The issue with plates and screws is that the clavicle is a bone very close to the skin therefore in most patients the plate is prominent and can be painful leading to up to 20% of patients requesting it being removed. When removed, each screw hole is at risk for another fracture until the holes heal, which can take another 3 months.
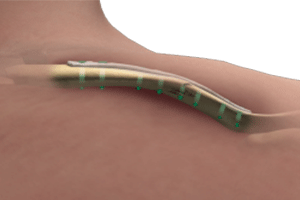
A new alternative to plate and screws is a rod that can be placed inside the clavicle through a minimally invasive technique that avoids the large painful incision of plates and avoids the risk of re-fracture later even if removed.

In summary, if you suffer a clavicle fracture you should see an ORTHOPAEDIC specialist within days of your injury. The X-rays need to be carefully examined as often the initial screening X-ray in the emergency room does not adequately show the fracture pattern. The treatment options should be discussed, with future function of the shoulder region a priority. Avoidance of a fracture that doesn’t heal or heals in a bad position is of utmost importance for your future function and satisfaction.